Desmoid Fibromatosis
Epidemiology
- Desmoid fibromatosis is arbitrarily divided into two types: anterior abdominal wall and extra- abdominal wall.
- The extra-abdominal variety, which is more common, is also known as musculoaponeurotic or aggressive fibromatosis.
- The histologic appearances of these varieties are the same.
- Approximately 1 0 to 30% of all extra-abdominal desmoids are found in the head and neck.
- Desmoid fibromatosis affects a wide age group ranging from infants to the eighth decade.
- Most patients, however, are in the third and fourth decades.
- There is no sex predilection for the extra-abdominal variety although there is a female preponderance in the abdominal type.
Clinical Findings
- The lesion is firm to hard and is characteristically slow growing.
- Most lesions are non-tender and painless.
- They may be noted ro develop in previously irradiated fields or surgical scars.
- Some lesions are multicentric.
- Lesions resemble scar and may be impossible to distinguish from proliferating scar tissue both clinically and pathologically.
Pathology
- The lesions are variable in size and may grow beyond 20 cm.
- They develop within muscles, aponeurosis, or fascia and typically infiltrate the muscles along the long axis.
- Microscopically, the muscles and aponeurosis are invaded by mature, uniform, spindle-shaped cells.
- The infiltrative process separates the muscle bundles and these muscles eventually show atrophy.
- In some patients these lesions turn sarcomatous.
Treatment
- Lesions of head and neck desmoid fibromatosis appear more aggressive than lesions elsewhere.
- They should be treated by wide surgical resections. Because of the infiltrative behavior, surgical clear margins are difficult to achieve.
- Hence, recurrences are common (20-77%), and most lesions recur within the first 2 years.
- Patients may die from aggressive local disease, and some patients may also have distant metastasis.
- Chemotherapy may also be successful in some patients using nonsteroidal anti-inflammatory agents, tamoxifen, and colchicine.
Imaging Findings
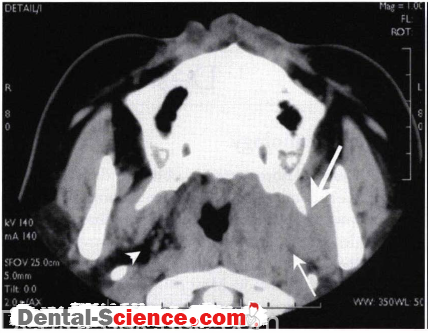
CT
- The CT findings of desmoid fibromatosis are nonspecific.
- These tumors show variable enhancement and cannot be distinguished from malignant infiltrative lesions
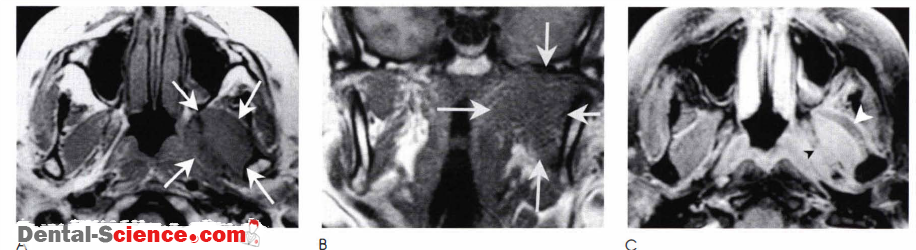
MR
- The MR findings are also nonspecific.
- Lesions show intermediate signal intensity on T I weighted images and high signal intensity on T2-weighted images.
- They enhance strongly after the injection of contrast
Imaging Pearls
• CT and MR imaging findings cannot distinguish desmoid fibromatosis from other malignant lesions.
- However, because of me slow growing process, bones rend to be remodeled rather than infiltrated .
• Desmoid fibromatosis may be multicenrric.
- Hence, separate masses in the head and neck may point toward this diagnostic possibility.
ــــــــــــــــــــ► ⒹⒺⓃⓉⒶⓁ–ⓈⒸⒾⒺⓝⓒⒺ ◄ــــــــــــــــــــ