Retromolar Carcinoma with masticator space spread
Epidemiology
- Oral and oropharyngeal carcinomas are usually seen in patients over 60 years old.
- In recent years these tumors have been increasingly encountered in patients who are in the 30’s, 40’s and 50’s.
- With the increased use of tobacco and alcohol by females, the male to female ratio of the incidence of oral and oropharyngeal tumors has changed from 1 0: 1 to 4: 1 .
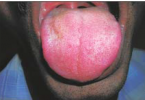
Clinical Findings
- Retromolar trigone carcinoma may present with pain or bleeding in the oral cavity.
- On examination, a mass in the retromolar trigone/anterior tonsillar pillar area may be evident.
- This lesion may be associated with dysplastic mucosal changes in the oral cavity.
- Patients with deep involvement of the muscles of mastication may also complain of trismus.
Pathology
- The retromolar trigone is located over the anterior aspect of the mandible behind the third molar.
- Laterall y it is bounded by the buccal mucosa, and medially it is continuous with the anterior tonsillar pillar.
- Although the retromolar trigone is anatomically located within the oral cavity, it behaves like an oropharyngeal malignancy.
- The tumor is usually poorly to moderately differentiated squamous cell carcinoma.
- It may erode the ramus of the mandible posteriorly; invade the tonsillar fossa, tongue base, and muscles of mastication medially; and extend to the back of the maxilla and pterygopalatine fossa superiorly.
Treatment
- Tumors that are small to moderate in size can be treated entirely with radiation therapy.
- However, invasion of the adjacent mandible requires surgical resection.
- Postsurgical radiation therapy may also be given
Imaging Findings
CT
- Like mucosal malignancies elsewhere, both CT and MR imaging underestimate the extent of mucosal involvement.
- The tumor shows moderate contrast enhancement.
- Early cortical erosion of the mandible is best identified with CT.
- Tumor can infiltrate the medial pterygoid muscle, spread superiorly to the pterygoid fossa, and continue to spread along the lateral pterygoid muscle.
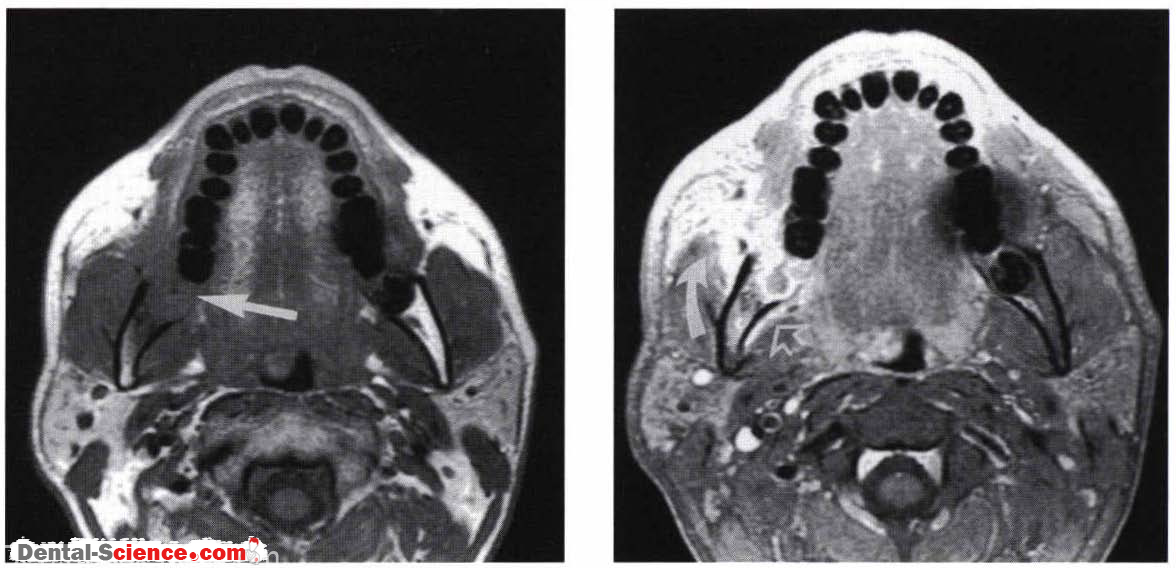
MR
- Deep infiltration of the masticator muscles shows good contrast enhancement.
- T2-weighted images typically demonstrate high signals.
- The high signal intensity mandibular marrow when replaced with tumor is readily seen on T I -weighted images
Imaging Pearls
• Perineural spread may take place when tumor invades the mandible and spreads along the inferior alveolar nerve to the pterygopalatine fossa and intracranially along cranial nerve V2 . Alternatively, tumor may spread directly to the pterygopalatine fossa and subsequently through the foramen rotundum .
• Perineural spread can also take place along cranial nerve V3. Because the muscles of mastication are innervated by cranial nerve V3, masticator space involvement may be followed by spread through the foramen ovale. It is therefore important to examine the course of both cranial nerve V 2 and V 3′
ــــــــــــــــــــ► ⒹⒺⓃⓉⒶⓁ–ⓈⒸⒾⒺⓝⓒⒺ ◄ــــــــــــــــــــ