Gingival Recession
Introduction
Gingival recession is characterized by the displacement of the gingival margin apically from the cementoenamel junction, or CEJ, or from the former location of the CEJ in which restorations have distorted the location or appearance of the CEJ.
Gingival recession can be localized or generalized and be associated with one or more surfaces.
The resulting root exposure is not esthetically pleasing and may lead to sensitivity and root caries
In USA, it was revealed that the prevalence of ≥1 mm recession in persons 30 years and older was 58%, representing 61.3 million adults, and the extent of ≥1 mm recession averaged 22.3% teeth per person.
The extent of ≥1 mm recession was 38.4% teeth per person among persons with gingival recession.
The prevalence and extent of recession increased steadily with the age of the cohort, regardless of the threshold level used in defining recession.
In the youngest age cohort (30 to 39 years), the prevalence of recession was 37.8% and the extent averaged 8.6% teeth.
In contrast, the oldest cohort, aged 80 to 90 years, had a prevalence of 90.4% (more than twice as high), and the extent averaged 56.3% teeth (more than six times as large).
A comparison by gender and race/ethnicity showed that the prevalence and extent of recession were significantly higher in males than females (P< 0.001) after adjusting for age and race/ethnicity, and in blacks than in whites (P< 0.002), after adjusting for age and gender

Factors related to etiology of gingival recession
Aging
Anatomical factors that have been related to recession include fenestration and dehiscence of the alveolar bone, abnormal tooth position in the arch, aberrant path of eruption of the tooth, individual tooth shape and presence/lack of attached gingiva
Physiological factors may include the orthodontic movement of teeth to positions outside the labial or lingual alveolar plate, leading to dehiscence formation.
Various forms of trauma—such as vigorous tooth brushing, aberrant frenal attachment, occlusal injury, operative procedures and tobacco chewing—have been thought to play a role in the etiology of recession.
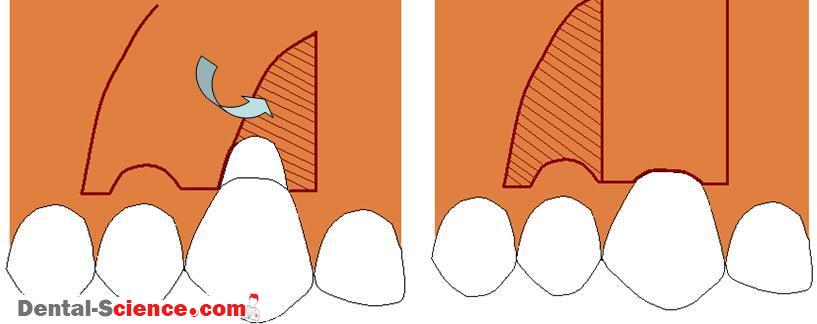
Classification according to Miller
Class I: Marginal tissue recession not extending to the mucogingival junction. No loss of interdental bone or soft tissue.
Class II: Marginal tissue recession extends to or beyond the mucogingival junction. No loss of interdental bone or soft tissue.
Class III: Marginal tissue recession extends to or beyond the mucogingival junction. Loss of interdental bone. Interdental soft tissue is apical to the cemento-enamel junction, but coronal to the apical extent of the marginal tissue recession.
Class IV: Marginal tissue recession extends beyond the mucogingival junction. Loss of interdental bone and to a level corresponding to the apical extent of the marginal tissue recession.
Limitation of Miller’s Classification :
The position of the tooth and the alveolar ridge are not taken into account. Recessions in teeth in a labial position may require orthodontic treatment prior to surgical procedures.
The size of the defect in both vertical and horizontal dimensions must be considered. As a rule of thumb, the literature classifies the defects as shallow (<3 mm), moderate (3 to 5 mm) or deep (>5 mm). On average, clinical studies indicate a defect width of 4.5 mm. A 5-mm width should be viewed as wide. It is to be assumed that the larger the recession area, the less root coverage should be expected.
The residual depth of the vestibule also seems to be of importance for the selection of procedures.
Index of Recession
A new two-figure Index of Recession (IR) was described by Smith (1997).
The horizontal component – the first digit – is expressed as a whole number value from the range 0-5 depending on what proportion of the CEJ is exposed, on either the facial or lingual aspects of the tooth, between the mesial and distal midpoints (MM-MD distance) approximally.
The criteria are as follows:
0; no clinical evidence of root exposure
1: as 0, but a subjective awareness of dentinal hypersensitivity in response to a 1 second air blast is reported and/or there is clinically detectable exposure of the CEJ for up to 10% of the estimated MM-MD distance: a slit like defect
2; horizontal exposure of the CEJ >I0% but not exceeding 25% of the estimated MM-MD distance
3: exposure of the CEJ >25% of the MM-MD distance but not exceeding 50%
4; exposure of the CEJ >50% of the MM-MD distance but not exceeding 75% 5: exposure of the CEJ >75’/o of the MM-MD distance up to 100%
Allocation of these codes does not imply that the extent of recession is equally dispersed about the facial or lingual midpoints of the area of exposed roots.
The second digit of the IR gives the vertical extent of recession measured in whole mm on a range 0-9.
The precise criteria proposed are as follows:
0: no clinical evidence of root exposure
1: as 0, but a subjective awareness of dentinal hypersensitivity is reported and/or there is clinically detectable exposure of the CEJ not extending >1 mm vertically to the gingival margin
2-8: root exposure 2-8 mm extending vertically from the CEJ to the base of the soft tissue defect
9: root exposure>8 mm from the CEJ to the base of the soft tissue defect.
An asterisk is afixed to the second digit whenever the vertical component of the soft tissue defect encroaches into the muco-gingival junction or extends beyond it into alveolar mucosa.
The absence of an asterisk thus implies either absence of muco-gingival junction at the indexed site or its non-involvement in the soft tissue defect.
The prefixed F (or L) denotes whether gingival recession is facial {or lingual) to the involved root.
ــــــــــــــــــــ► ⒹⒺⓃⓉⒶⓁ–ⓈⒸⒾⒺⓝⓒⒺ ◄ــــــــــــــــــــ