Aphthae
(Recurrent aphthous stomatitis – RAS)
Clinical features
– Recurrent ulcers.
– There are three distinct clinical patterns:
1. Minor |
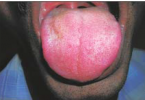
2. Major |
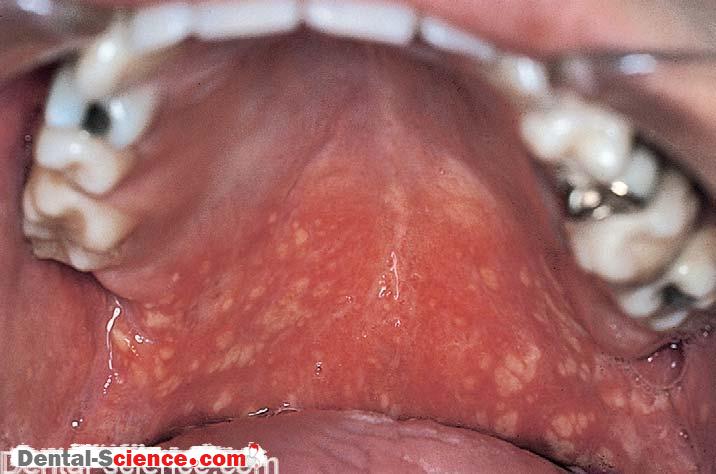
3. Herpetiform ulcers |
– Small ulcers (<4 mm) on mobile mucosa (mostly labial and buccal mucosae). – Less than five ulcers at one time. – Healing within 14 days. – Erythematous borders. – No vesicle formation. – No scarring. | – large ulcers (may be >1 cm). – any site including dorsum of tongue and hard palate. – Healing within 1-3 months. – With scarring. – Extreme pain and lymph node enlargement are common. | – Multiple (10-100). – Minute (1-2 mm) ulcers that coalesce to produce ragged ulcers. – Any part of the oral mcosa, more frequently tip of the tongue, labial mcosa, margins of the tongue. |
Incidence
– About 25% of population, mostly non-smokers.
Aetiology
– Unclear.
– No reliable evidence of autoimmune disease or any classical immunological reactions.
– May be cell-mediated immune responses with cross-reactivity between Streptococcus sanguis, heat shock protein and oral mucosal tissue.
– Underlying predisposing factors seen in a minority include:
– Haematinic deficiency (iron, folate or vitamin B12) in 10-20%.
– Relationship with luteal phase of menstruation (rarely).
– Stress.
– Food allergies.
– HIV disease (major aphthae).
– Some drugs.
– Onset is usually in childhood or adolescence.
– Later onset may signify haematinic deficiency or HIV disease.
Diagnosis
– Diagnosed from history and clinical features.
– A blood picture is useful to exclude deficiencies.
– There is no diagnostic test of value.
– Differentiate from other causes of mouth ulcers, especially Behçet’s syndrome.
Management
– Treat any underlying predisposing factors.
– Treat aphthae with chlorhexidine 0.2% aqueous mouthwash or topical corticosteroids (hydrocortisone hemisuccinate 2.5 mg pellets or 0.1% triamcinolone acetonide in orabase) or tetracycline rinses.
– Rarely, more potent topical steroids or other agents such as thalidomide may be needed.